Zero Net Energy Without Adding Zeros to Cost
Reaching an ambitious sustainability goal at Bristol Community College


A recent front page article in The New York Times paints a striking image of Northeast Ohio’s economy. Manufacturing jobs, long the calling card of the region, saw a decrease of some 40% since 2000, while healthcare jobs have spiked 30% in the same period of time. This shift, though perhaps more pronounced in the Rust Belt, has taken hold all across the country. The implication is clear: the healthcare industry has become a major engine for our national economy, often filling in the gaps left by other industries.
This growth doesn’t stop at the hospital’s door—the increased economic importance of healthcare is transforming the educational landscape, too. The industry’s growth necessitates academic health science programs that can train a steady stream of practitioners—from doctors and nurses, to EMTs and hospice care providers. These programs will be critical in meeting current demand and projected shortages in the talent pool. One recent article in The Atlantic cites that 1.2 million openings for registered nurses alone will open up between now and 2022.
This growing demand is certainly not lost on schools. Leading schools in this space are instituting cutting-edge programs that blur the lines between research, clinical practice, and technology. Many schools are starting new, or expanding existing, nursing and med-tech allied health programs. Many programs are turning traditional teaching methods on their heads to better enable graduates to hit the ground running as they leave the classroom behind and step into the hospital ward setting. Whatever form they take, the proliferation of academic health science programs, and the opportunities awaiting their graduates, has impacted practically every corner of the country.
To fully capture the possibilities of expanding academic health sciences, institutions must consider many angles and multiple scales: from a region’s economic policies, to the history and organization of a campus, all the way down to an individual building and its mix of labs, classrooms, and informal space. There is no one-size-fits-all solution—a simple fact that liberates each institution to celebrate their unique identity and focus on their own strong suits. Below, Tyler Patrick explores important factors to consider in defining the settings for hands-on medical education and training, through the lens of pedagogy, campus planning, and design.

Students at Methodist University’s Thomas R. McLean Health Sciences Building practice hoisting a simulation robot onto a stretcher

Simulation classrooms enable students to synthesize the theoretical with the applied. Here, two students interact with an actor in a realistic exam room setting
By Tyler Patrick, AICP. Patrick is a Sasaki planner and principal who has managed a wide range of campus planning efforts throughout the nation. He is dedicated to creating achievable planning solutions and seeks to advance the academic mission of the colleges and universities with which he works.
Recent evolutions in health science education have made campus planning more important than ever. As programs increasingly mix and mingle, the traditional divisions of space begin to blur. What spaces will enable these integrated environments to thrive? Are some spaces unnecessary or redundant? By analyzing a school’s existing health science programs, we can uncover mutual interests, overlapping pedagogies, and demands for similar types of spaces. In this way, the planning process helps identify the specialized needs that support different disciplines, as well as latent opportunities for sharing space and equipment.
There are myriad considerations to look at in any planning project. For the purposes of this article, let’s look at two categories: stakeholder input and spatial analysis.
Stakeholder input is an indispensable part of developing a successful master plan. We continue to iterate our approaches to gathering this feedback, developing a specialized kit of tools that enable us to gain insight into an institution’s goals, or to shed light on underlying issues holding them back from success. Our Collaboration Survey, for example, allows us to identify how individuals work with one another across traditional departmental boundaries, both today and aspirationally in the future.
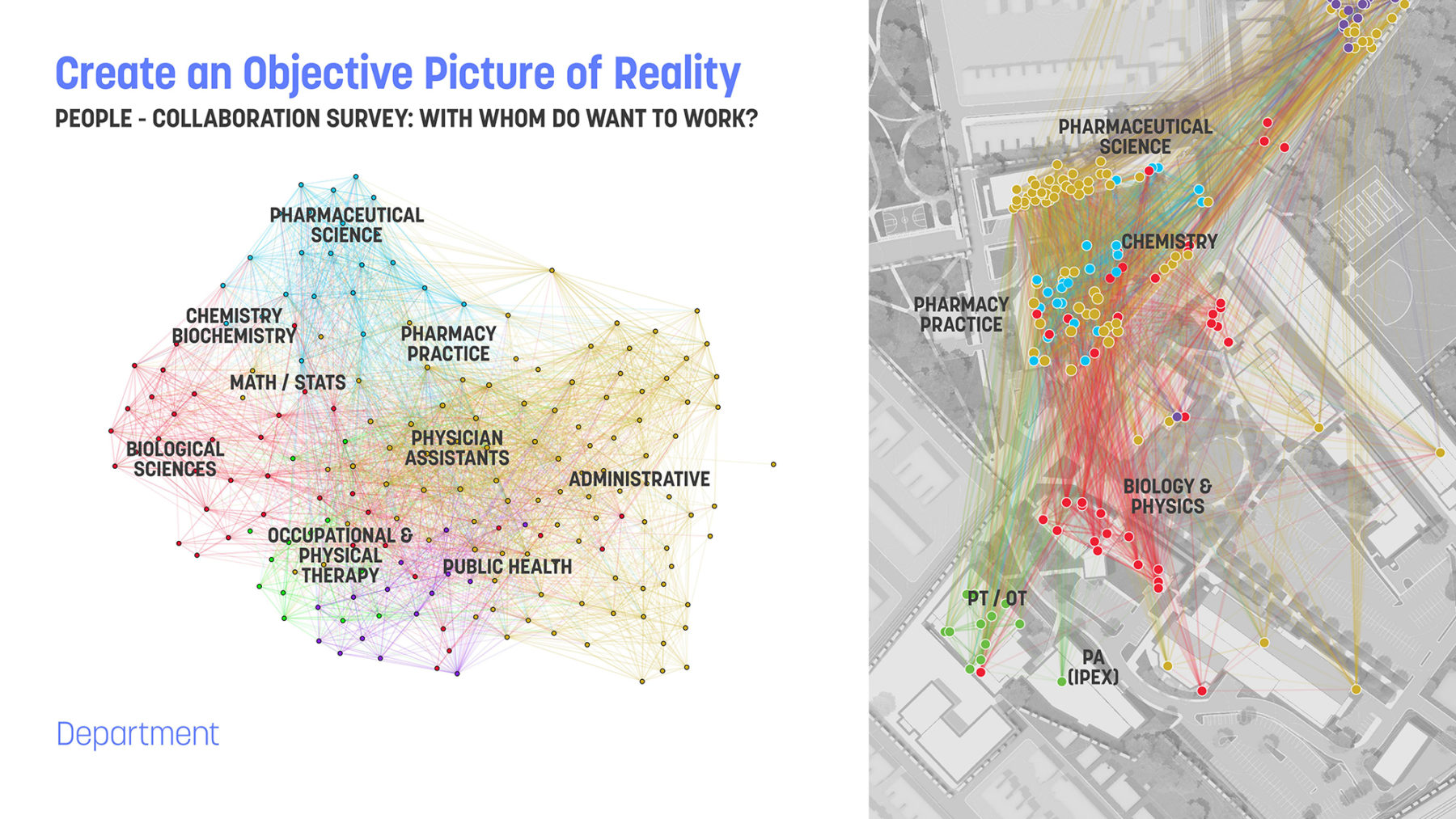
Data from a Collaboration Survey for the University of Sciences in Philadelphia. Each respondent is shown as a dot, while the lines show each instance of collaboration within and across disciplines
Quite often, individuals work across departmental boundaries to address thematic issues. This is especially true in the health sciences, where research into a particular disease may involve more than one health science discipline, or might address broader issues, such as the patient experience. Once we understand the nature of these collaborations, we can explore the potential physical implications of such collaboration. Does collocation make sense? Are there ways to optimize shared, core facilities? Are there opportunities for hoteling or touch-down space that encourage serendipitous encounters?
Before you can confidently plan new spaces, you have to have a clear understanding of the spaces you already have. When looking at existing space, traditional space data only goes so far. The data can tell us a lot about the quantity of space, or the intensity of the use of space, but we often don’t get a sense of the quality of space. Most qualitative space analyses are done at the building level, and they focus on things like infrastructure, and exterior building conditions. These are all important categories, but they don’t provide the full picture.
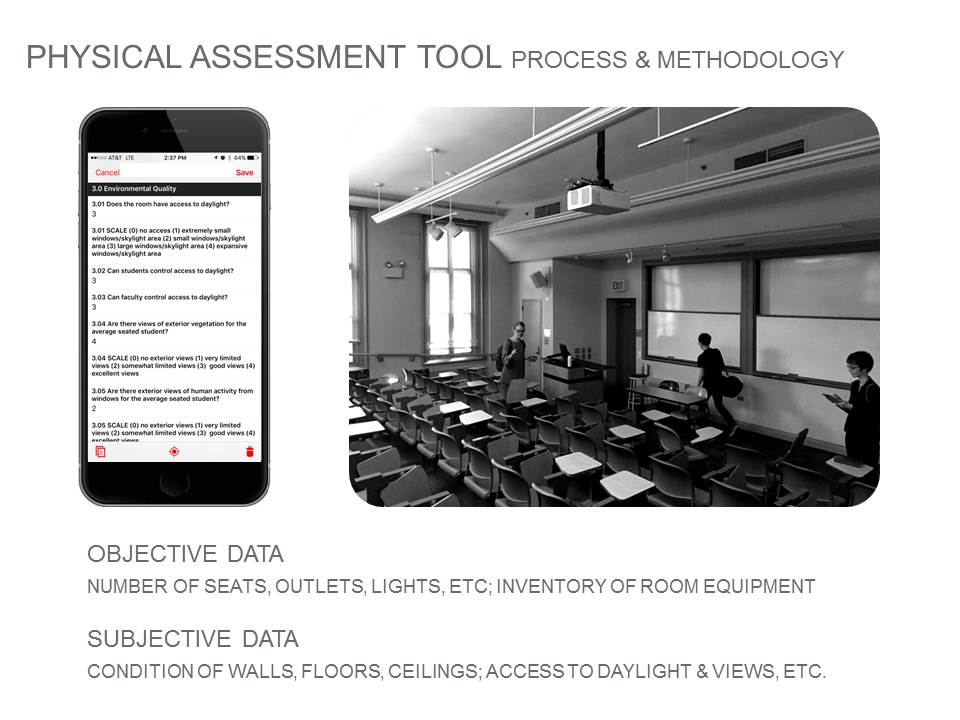
We use a custom-built mobile app to grade every room along objective and subjective parameters of quality
In our learning space and health science master plans, we assess each room to understand its performance relative to environmental considerations, furnishings, technology, and layout. By assessing these characteristics, we understand more about the learning environment, not just the general architectural or infrastructure components of space. We can then use this information to understand and determine the extent to which a relationship exists between use of space and condition of space.
Combined, these quantitative and qualitative analyses paint a more holistic understanding of existing conditions and allow us to formulate customized and specific strategies for renovation and reuse. This is why it’s so important to link planning and analysis to architecture. We work along this continuum, providing specific implementable solutions to the issues we uncover during the analysis phase.
One way in which we source feedback during the design process is through our MyBuilding survey. The survey visualizes qualitative data on how stakeholders use the spaces within an existing building—often revealing space shortages, abundances, and unexpected uses. The data output from this survey helps leadership make informed, confident design decisions. While there are many other variables that impact the design of academic health science buildings and spaces, designers must play their part. The best solutions come from objectively understanding the client’s real needs, and that understanding can only be gained through listening.